had barely begun bat mitzvah lessons when my womanhood arrived early in the form of a training bra. Still practically concave, Limited Too knew just what to do to convince me I meant nothing without it.
Introduced in the 1950s, training bras were touted by doctors as a preventative measure. A prophylactic of sorts for saggy breasts inadequate for nursing future babies. This timing, uncoincidentally, aligned with Hollywood's fixation on full-breasted women like Marilyn Monroe and Jane Russell.
This useless mini camisole draped over barely there breast buds quickly became an essential component to the puberty starter pack, and breasts in turn became a defining component of femininity. This became especially difficult for the population most frequently losing their breasts in the mid to late 20th century: women with breast cancer. A 1996 New York Times' article titled "Women Who Lose Breasts Define Their Own Femininity," begins by lamenting for the women of the 1960's and 1970's who worried "the loss of a breast would somehow diminish their femininity and sexual attractiveness" if they survived the disease. Women like my grandmother, who had a single mastectomy in the late 1970s and has worn a prostheses every day since.
"Today," the article says, "women are less likely to perceive breast cancer as an attack on their innate feminine nature."
Nearly two decades later, The Cut published "Angelina Jolie: Breasts Don't Define Femininity." When sex symbol Angelina Jolie got a preventative double mastectomy and wrote about it in the New York Times, the implied message, according to The Cut, is you can be a normal woman without natural breasts or even with no breasts at all. But Jolie got high quality breast reconstruction indistinguishable from a natural breast to an untrained eye.
It seems that nearly 70 years after the full-breast boom, women are unsuccessfully trying to convince ourselves we've reclaimed the power over our femininity.
But not for much longer.
"I identify as a woman, but I have just redefined what woman means," said Molly O'Handley, a production assistant and restaurant server.
O'Handley underwent top surgery on April 26. Top surgery refers to a variety of procedures that make the chest appear less like the gender identity the patient was assigned at birth. For O'Handley, this means a double mastectomy.
Photo Source: Molly O'Handley
Having earned my bachelor's degree in gender and sexuality studies, and having to simply exist as a lesbian, I'm well accustomed to encountering the confusion and shock in the face of "new" identities or behaviors like a cisgender woman wanting to remove her breasts. But O'Handley was the third cis woman I met in a six-month span who had gotten or was actively pursuing top surgery. In fact, nearly all the people I profile in this piece are friends or folks I met through friends. And each time I brought top surgery up in my queer circles I realized how prevalent, yet mostly unmentioned, the procedure is.
This chronic perception of newness regarding non-normative expressions of gender and sexuality is not only wrong, it's dangerous. Newness makes identities such as nonbinary or genderqueer seem like trends, erasing the histories necessary to remember that gender norms are always in flux—ender norms like the hypersexualization and feminization of breasts that O'Handley spent years of work unlearning.
"I was trying to disconnect my self-worth from the male gaze," O'Handley said. "My tits were how I would describe my worth because of the way that men would look at me since I was so developed."
The hypersexualization of breasts is so common it's accepted as natural. Little girls are told to cover their chests before they even develop. Breasts can be plastered all over Instagram and Facebook, as long as the nipple is covered up, but breastfeeding mothers are told to cover up. Breasts are synonymous to womanhood, and women are inherently sexual. If O'Handley's worth was measured by her breasts, what would she be worth after removing them?
"I'm worth so much more than anyone else's opinion," said O'Handley. "Once I started to think about that, I began to feel more in line with what I actually want, which is this."
While hundreds of thousands of women every year receive breast implants with little difficulty, people across the gender spectrum who wish to do the opposite are confronted by a health care system and a society that challenges the validity of their identity each step of the way. Insurance companies and medical providers pathologize patients, often outlining strict access guidelines or simply refusing to provide care.
But O'Handley's redefined woman is indicative of a burgeoning countermovement. The fight to reclaim breasts from this sexualized, gendered narrative in order to have the autonomy to remove them is forcing medicine, and in turn society, to question narrow gender norms in the process.
Making the Decision
O
ne major indicator of this countermovement is the steady increase of patients seeking gender affirmation surgery. The American Society of Plastic Surgeons reported over 3,200 gender-affirmation surgeries in 2016—a 20 percent increase from the previous year.
The 2015 U.S. Transgender Survey, the largest survey examining the experiences of transgender and nonbinary people with nearly 28,000 respondents, found high rates of what they refer to as "chest reduction or reconstruction" surgery. Among trans men, 97 percent had either had or are planning to have the surgery and the remaining 3 percent are unsure. Among nonbinary people with female on their original birth certificate, 6 percent had the surgery, 42 percent want it and 31 percent are unsure.
While this growth is largely tied to increased insurance coverage of the procedure and surgeons trained and willing to perform it, there are important social and personal experiences that lead people to pursue top surgery in the first place.
As O'Handley points out, the connection of breasts to a woman's worth can make top surgery an unlikely consideration for people who don't identify as strictly female-to-male (FtM).
Talayeh Nasirzadeh, a personal assistant to a musician and one of my first friends in Los Angeles, first heard about top surgery from a college friend who is trans. Nasirzadeh, who identifies as a cis women, did not yet consider this could be something she would pursue. "Because the guy who educated me about the procedure was trans, that made sense to me because it fit what we're taught is normal," Nasirzadeh said. "So I always associated it with transitioning."
Photo Source: Talayeh Nasirzadeh
Similarly, Israeli teacher and drag king Lee Arnon, who I met through my girlfriend, learned about the procedure 11 years ago from their high school best friend who had come out as trans. "At that time I didn't think of getting it done because I'm not a trans man," Arnon said. "It took me years after that to come out as nonbinary."
Celeste Monsour, a market research analyst in Florida who I found through YouTube, had also only heard about top surgery in explicitly FTM contexts as well until they discovered the blog Neutrois Nonsense. Run by Micah Rajunov, a nonbinary person who documented their experience with top surgery, this blog piqued Monsour's curiosity. "It took a couple more years for me to identify as nonbinary," they said. The turning point came when Monsour tried binding.
Chest binding involves compressing breasts with methods including commercial binders, elastic bandages, duct tape or plastic wrap to create a more masculinized chest appearance. A vital daily ritual for many people experiencing breast dysphoria, binding's positive impact on emotional and behavioral health is in tension with the physical discomfort and possible long term health complications. In a 2016 binding study, the first to be published in a medical journal, over 97 percent of the 1800 respondents reported at least one negative health outcome ranging from back and chest pain to shortness of breath and fractured ribs.
Unable to bind regularly due to chronic migraines triggered by the restricted breathing, Monsour reserved binding for cosplay conventions. "This was my way of doing it without it being a weird gender thing I'd have to explain," she said. "Even though it was restrictive, binding made me feel less restricted - like there was less holding me back from just moving around and doing stuff even though there was something that was actually doing that."
At that point Monsour realized they could no longer "pretend to be okay" with their chest and began seriously considering top surgery.
I didn't feel like I could be myself, or be the best version of myself, without the binder.
Like Monsour, O'Handley and Arnon cite binding as integral to their decision making process. O'Handley was binding for three years before stopping recently due to the pain. "I didn't feel like I could be myself, or be the best version of myself, without the binder, so I'm so happy I'm getting this surgery," she explained.
Arnon began binding when they started drag 10 years ago at 17. "I realized I felt better when my chest was bound, so it became a part of me," they said. When Arnon joined the Israeli Defense Force at 18, the baggy uniforms assuaged their breast dysphoria enough to get by during their seven-year service.
But, upon leaving the army three years ago, Arnon's dysphoria worsened and they began to question what identity felt true to them. "I started to ask myself questions like, 'am I a man? Woman? What's good for me?' And I realized both were wrong, because I don't feel like either," they said. "What I did understand is the part I felt most uncomfortable with was my chest." Dreading any situation involving chest exposure, including necessities like showering, Arnon decided on top surgery.
For Nasirzadeh, who doesn't bind due to the health risks, the realization that top surgery could apply to her came after losing a significant amount of weight three years ago. Feeling more comfortable in her body than she ever had before, she realized her discomfort with her chest remained the same. "The area still just doesn't make sense for me," she explained. "Then I met someone similar to me who said they got the surgery because they just didn't like having titties and I was like, 'Oh fuck yeah. I'm really behind that idea.'"
Once the personal decision to pursue top surgery is made, the next step is coming to terms with telling others. The visibility of people who have already had top surgery is a crucial component for many in alleviating stigma and finding resources and community support. O'Handley, for example, said meeting more people who had gotten the surgery, including two close friends, made it "more and more apparent that I was allowed to feel however I wanted to feel."
For the many people who need these moments of clarification and validation but are geographically isolated, a vast network exists online in messaging forums like Reddit and Tumblr as well as in the comment sections of YouTube top surgery vlogs. Jason Boyask, a trans activist and the reigning Mr. Philadelphia Leather 2019, relied heavily on vlogs trans men posted documenting their transitions. When Boyask got top surgery nine years ago at 16, these vlogs were a vital resource fulfilling both educational and emotional needs.
Full disclosure: Boyask and I went to college together, where we co-founded the Queer Advocacy Group along with some friends. Together we convinced [forced] our school to open gender neutral bathroom and housing options. He's someone I've shed quite a few tears with.
"I've had some really beautiful full-circle moments where some of the people whose blogs saved my life and helped me discover who I am have been people I've been able to meet and become friends with," Boyask said.
Click for YouTube Video
Photo Source: Celeste Monsour
These interactions are what motivate Monsour to share their own experience with top surgery as a nonbinary person. For Monsour, visibility is important to help people considering top surgery educate themselves, as well as their family and friends. Having relied on top surgery vlogs when discussing the surgery with their parents, Monsour now wants to empower others with the tools to say, "look. Here's somebody who's done this. It's not some wild thing I've just made up. This is how it works and I have seen it turn out well for people."
Even with the help of vlogs, explaining the vastness of gender identity to family unfamiliar with the language is no simple task.
For O'Handley, explaining her decision meant demonstrating this was not "out of the blue," as her mother questioned, and that she could still be a woman without her breasts. "It felt sudden to my parents because they're far away—they don't see me binding every day or know I've been going to therapy for two years like my friends do," she said. "I told my mom it's just not a part of my body I relate to, but it doesn't mean I'm not a woman, because that means something different for every person."
"I think that's what hard for people, is recognizing that there's no fixed anything," O'Handley added.
Increasing visibility and community support is enabling more people across the gender spectrum to discover and embrace top surgery as a possible solution to breast dysphoria. But for many people, the process ends there.
Pre-Op
A
ccess to gender-affirming care in America is insufficient at its best.
The predominant barriers to care include lack of adequate insurance coverage, mistreatment or discrimination from health providers and the inexperience and discomfort of health providers treating transgender or nonbinary people. And, like trans and nonbinary identities themselves, this care inequity is nothing new.
"Medicine is always late to the game, especially around stuff like this," said Greta LaFleur, Assistant Professor of American Studies at Yale University.
A cultural historian whose work focuses on science, sexuality and queer studies, LaFleur maintains that "building a historical consciousness is important to understand our contemporary moment, of the politics of gender and sexuality in the here and now."
LaFleur described the intensified medicalization of trans and nonbinary people towards the end of the 19th and beginning of the early 20th centuries when "sexologists and psychiatrists started aiming their inquiries at what they called 'inverts'—people who suffer from inversion—who are trans people and queer people."
This history is key to understanding why top surgery is so inaccessible. Rather than focus on treating breast dysphoria by providing access to services such as hormone therapy and top surgery, the health care system pathologizes the whole person.
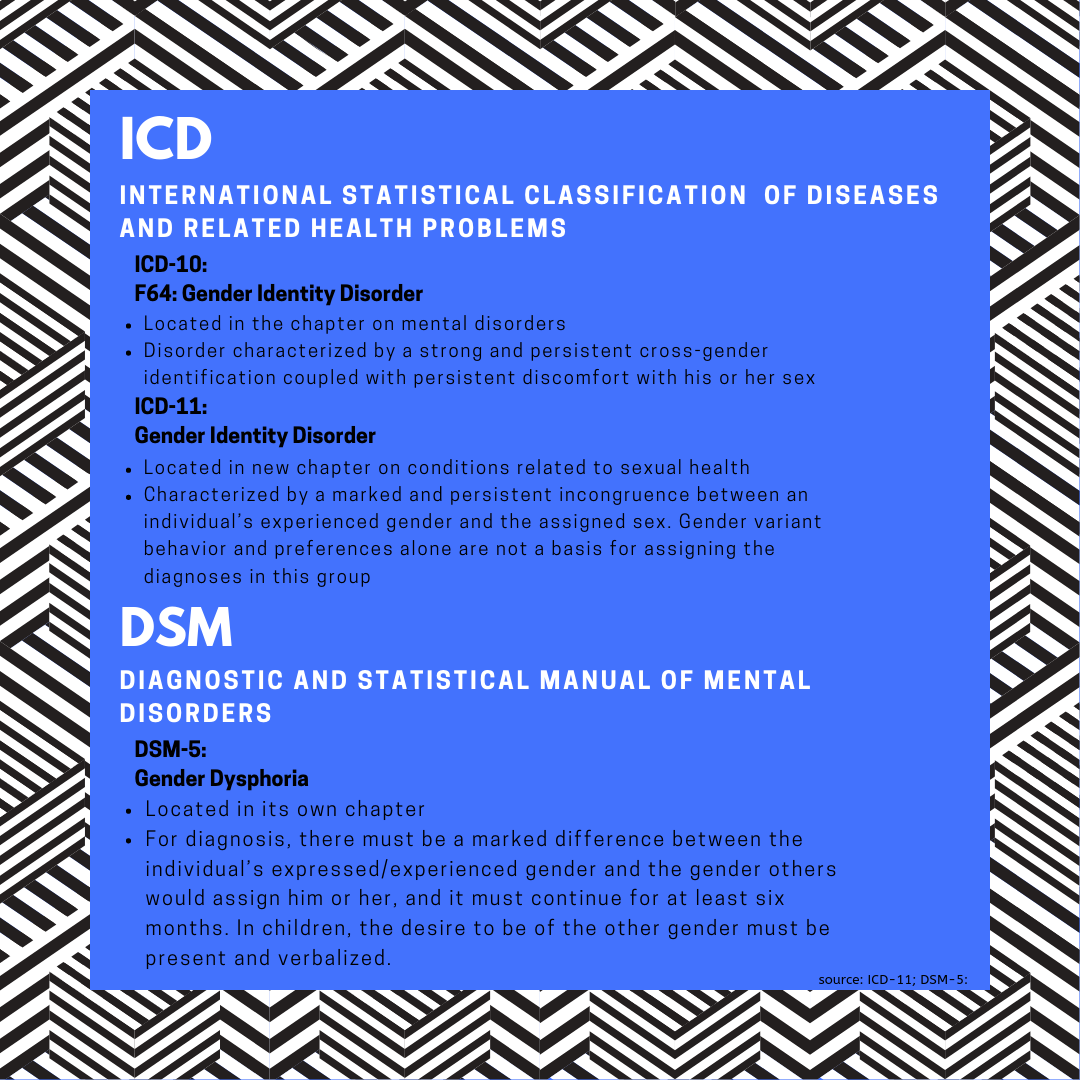
For most patients, accessing top surgery requires a diagnosis of gender dysphoria. Criteria for diagnosis are defined by two classification systems, the International Statistical Classification of Diseases and Related Health Problems (ICD) published by the World Health Organization and the Diagnostic and Statistical Manual of Mental Disorders (DSM) published by the American Psychiatric Association.
The U.S. currently relies on edition ICD-10 and DSM-5. Both systems still situate dysphoria within the gender binary using "his" and "her" pronouns, effectively erasing nonbinary identities from diagnostic criteria. ICD-10 also classifies gender dysphoria as a mental disorder called "Gender Identity Disorder," something DSM did away with in 2013.
CLICK TO ENLARGE
ICD-11, which will go into effect in January 2022, reclassifies Gender Identity Disorder as "Gender Incongruence," and removes the term from the chapter on mental disorders. This shift in terminology and perception is incredibly important, as ICD and DSM coding has profound consequences on provision of care, financing and insurance, and stigma. Adoption of ICD-11 in the U.S., however, will likely take much longer; ICD-10 was released in 1993 and was not implemented in the U.S. until 12 years later in 2015.
For clinical guidance in treating trans and nonbinary people, most health providers and insurance companies turn to the World Professional Association for Transgender Health (WPATH). Problematically, WPATH's most current Standards of Care, SOC-7, was published nearly a decade ago and much of it is now out of date by current community standards.
Many providers and insurance companies are using the "strictest WPATH guidelines from 2010," said psychologist Dr. Ruben Hopwood, coordinator of the Transgender Health Program at Fenway Health. "Then they apply these strict guidelines to everything, which makes it untenable."
Insurance companies have only recently entered the trans health care market, with San Francisco's July 2001 Transgender Benefit roll out being the first notable shift. Hopwood described how insurance companies charged the city "incredibly high fees" before having to, with legal force, admit "gender-affirming care wasn't costing them anything at all and completely removed any add on fees." With data on their side, trans health advocates were able to begin pushing insurance companies for coverage.
Around 2008 Hopwood himself began pushing Fenway Health, an LGBTQ health center, to include gender-affirming coverage in their employee insurance plans. After four years of work, Fenway Health and insurance provider Blue Cross Blue Shield rolled out Policy 189—the most comprehensive gender-affirming coverage in the country boasting 100 percent reimbursement and no lifetime caps that extended nationwide. "And it took four years to do that with a cooperative insurance company," Hopwood added.
Since then, many insurance companies have added some form of gender-affirming care coverage to their plans. Significant to this expansion is Section 1557 of the Affordable Care Act, which bans discrimination based on race, color, national origin, sex, age or disability in federally funded insurance plans and health care facilities. In 2016 the U.S. Department of Health and Human Services clarified that the ban on sex discrimination includes discrimination based on gender identity.
Despite this expansion of insurance coverage, a majority of patients still lack access to top surgery due to high insurance coverage variation, strict approval guidelines and discriminatory practices.
"A lot of insurance requires the individual to be trans and essentially living and identifying as the opposite gender and taking hormones for them to consider surgery," said Dr. Zol Kryger, a plastic surgeon who frequently performs top surgeries.
CLICK TO ENLARGE
As with any medical procedure, getting insurance to cover the costs requires proving medical necessity, and the medical necessity for top surgery is gender dysphoria.
"This is about proving someone's breasts are causing a functional impairment," Hopwood said. Unlike any other insurance-covered procedures, patients need to provide letters from both their medical provider and mental health provider to prove medical necessity.
"There's no good reason people should even have to have a therapy letter anyways, because the medical provider is providing a medical referral which is appropriate in every other case," said Aydin Olson-Kennedy, a licensed clinical social worker and Executive Director of the Los Angeles Gender Center. "That additional letter is largely to cover the surgeon's ass, so if the patient comes back saying they regret it then the surgeon won't get sued."
For mental health providers like Olson-Kennedy, himself is a trans man who had to navigate this same process a decade ago, patients can come in for a single consultation and leave with a letter. "There is no number for the length of therapy in WPATH," he explained. "Providers are arbitrarily deciding what the best number is and what many mental health and medical providers are really doing is saying, 'how many times do I have to see somebody before I am comfortable with OK-ing this.'"
The therapy letter requirement speaks to the deeply ingrained practice of pathologizing non-normative gender identity in the health care system. While many providers play into this discriminatory practice, others like Hopwood, Kryger and Olson-Kennedy have used their position to come up with creative ways to get patients covered.
"Sometimes from an insurance standpoint we'll request a breast reduction," Kryger said. "There is a sort of spectrum where a reduction becomes a full mastectomy." Whether the bill that goes to insurance says reduction or mastectomy, "the actual procedure focuses on addressing what that person wants," Kryger explained. "I'm never going to give a patient the wrong type of surgery because insurance wants to classify it as one thing or another."
This creativity is especially necessary for nonbinary people or cis women like O'Handley, who got her letter from Hopwood's Transgender Health Program at Fenway Health. "My therapist just used my name or 'the patient' instead of she/her pronouns," O'Handley said. "Insurance needs you to be trans enough, and I'm not trans, but I need this done."
Hopwood explained that providing care for nonbinary patients,"is where insurance companies get confused—they are starting to understand transgender within the binary but anything else they think the patient is just confused and needs to pick either male or female," Hopwood said. To bypass this, he and his colleagues will avoid putting pronouns in the therapy letter altogether.
This plan worked for O'Handley, who was quickly approved under her MassHealth insurance plan. While she'll have to pay for some expenses including medical tape and medication, the surgery itself will only cost her $50.
Referring to the care she got at Fenway Health, O'Handley said she feels "lucky to have doctors and therapists at a queer clinic who could tell me what path to take and language to use to get what I need."
And if insurance denies the patient, which frequently happens, Hopwood is adamant about going through the appeals process. "And if they deny you a second time, you have to appeal again because it's that third appeal to any insurance company when they're forced to be reviewed by someone outside the company, which has a higher likelihood of success."
For people who can afford to avoid this process, that is often the obvious choice. When Monsour realized they would have to pay nearly the full price for top surgery out of pocket, they chose to bypass insurance altogether. "I didn't want to have to go through all of that just to save a tiny bit," they said.
Photo Source: Jason Boyask
When Boyask got his top surgery nearly a decade ago, however, insurance was not even an option. And even without insurance, he still had to submit letters from both a medical provider and therapist before getting the surgery. "That is nuts to me, because any other form of plastic surgery you don't need therapy," Boyask said. "So if I'm not going through insurance then why?"
Ten years later, this is still the case for most patients who pay out-of-pocket. Arnon, who flew from Israel to get their surgery in Cleveland, Ohio, needed to provide a therapist letter as well.
Olson-Kennedy believes the predominant reason for this is "we still look at gender through the lense of choice." When people get nose jobs or breast implants, they're "probably doing that to enhance appearance to be more in line with very cisnormative experiences of body and attractiveness so we don't have feelings about that." But when that plastic surgery "goes against what is considered the social-political norms of secondary sex characteristicsor even just sort of bodies—then our values are like 'oh, but that's a choice.'"
Some surgeons have begun applying the informed consent model, traditionally used for elective surgery, to allow patients paying out-of-pocket to access top surgery without a therapy letter. "Informed consent looks like a natural conversation Dr. Mosser has in a gender-affirming environment to explore why the patient wants top surgery and what their goals are," said Charity Rose, director of transgender community engagement at the Gender Confirmation Center of San Francisco. Run by Dr. Mosser, cofounder of the American Society of Gender Surgeons, the Gender Confirmation Center provides top surgery for patients across the gender spectrum.
We still look at gender through the lens of choice
When neither insurance nor paying out of pocket are viable options, people can turn to grants and loans as another potential payment option. Mosser is a sponsor for Point of Pride, a scholarship-like program that provides direct financial assistance to trans people who cannot afford gender-affirming surgery. This year, Mosser is donating three surgeries which he will perform free of charge to patients connected with him through Point of Pride. For loans, Rose points to CreditCare, which is a medical financing company that works similarly to a credit card and carries steep interest rates hovering around 30 percent. CreditCare requires patients to have a good credit score and penalizes late payments with hefty fees.
Lastly, with all aforementioned payment sources coming up dry, people turn to crowdfunding sites like GoFundMe to cover the procedure. Simply typing "top surgery" into GoFundMe's search bar pulls over 22,000 hits, providing some scope for the number of people unable to access the procedure. O'Handley is using GoFundMe to cover non-surgical expenses including a compression binder needed for proper healing, medication and time off work.
If reading this section made you tired, image living it for years attempting to access care. Viewing breasts as a key component to femininity has been so naturalized that anyone seeking to severe that connection is treated with the utmost suspicion.
There is a difference—a vital difference—between wanting and needing cosmetic procedures, that practitioners and insurance companies often fail to notice. When people are barred from accessing gender-affirming care for a part of their body causing functional impairments, this can result in feelings of hopelessness and isolation and increased rates of anxiety and depression, Hopwood explained.
Surgeons themselves can play a critical role in securing funding for their patients' top surgery, however not every surgeon who performs the procedure provides gender-affirming care.